It’s been a whirlwind since posting here, and it has a lot to do with school (and thesis) starting, but also from my summer wrapping up work (and not finishing those Creative Summer tasks…whoops.)
I spent the summer working at Memorial Sloan Kettering Cancer Center, a cancer hospital here in NYC. As a Design Fellow on their Strategy & Innovation team, we were tasked to look at the Financial Toxicity of cancer care.
What is financial toxicity, you ask?
It’s a fancy way of saying that the cost of cancer care is astronomical, and has an adverse affect on one’s health.
Essentially, we were tasked with researching how awful it is to get a bill when you’re going through the worst health crisis of a person’s life. Sounds easy, right?





I, along with two other grad students from Parson’s SDM program and SVA’s Objects of Design, launched into it with three months to figure things out.
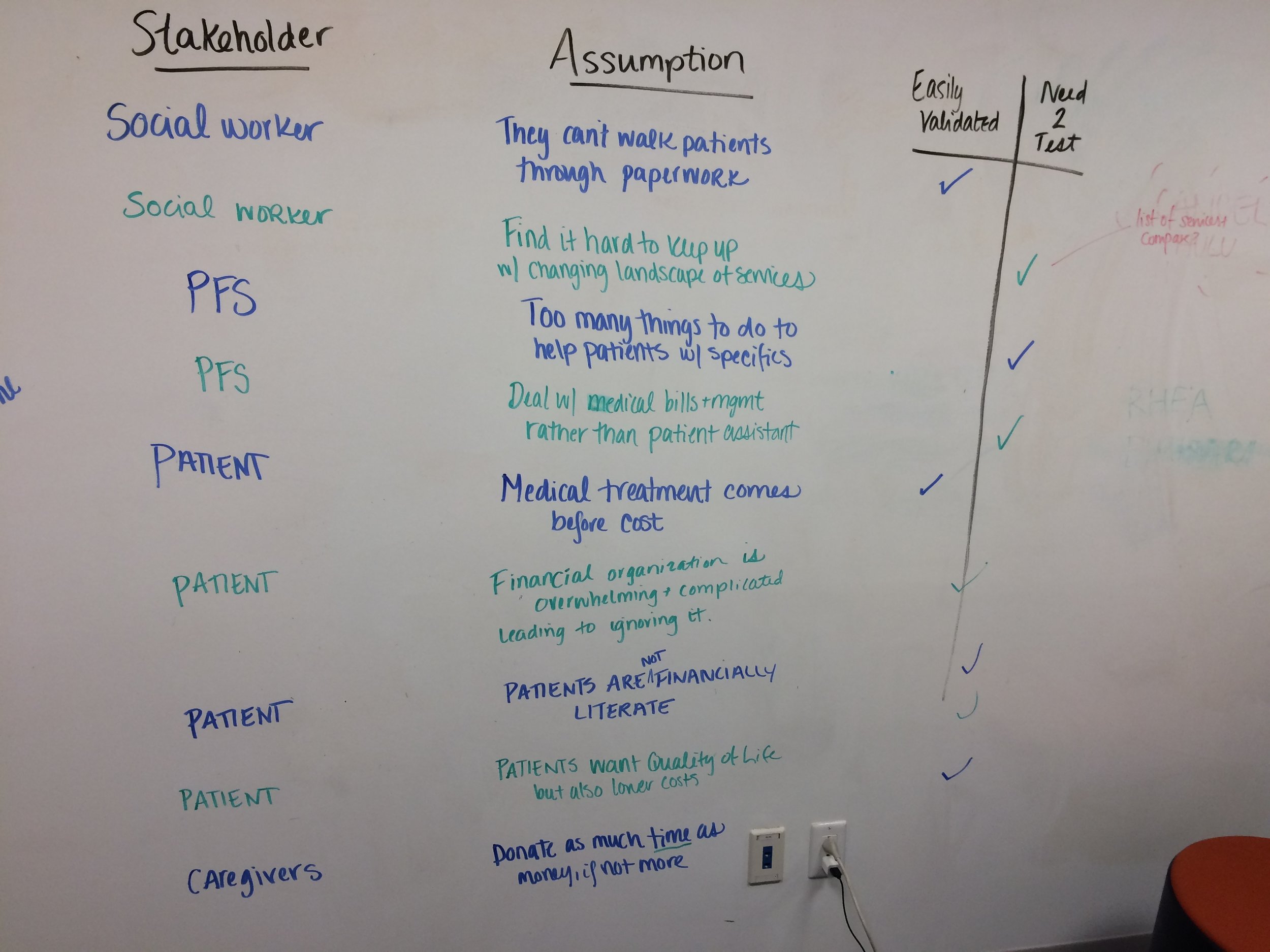
We conducted interviews across MSK, shadowing doctors on rotation, working with the Food Bank. and chatting with survivors about their financial woes. We did desk research, looked at the history of insurance and bills in health care, and mapped a lot. A lot a lot.

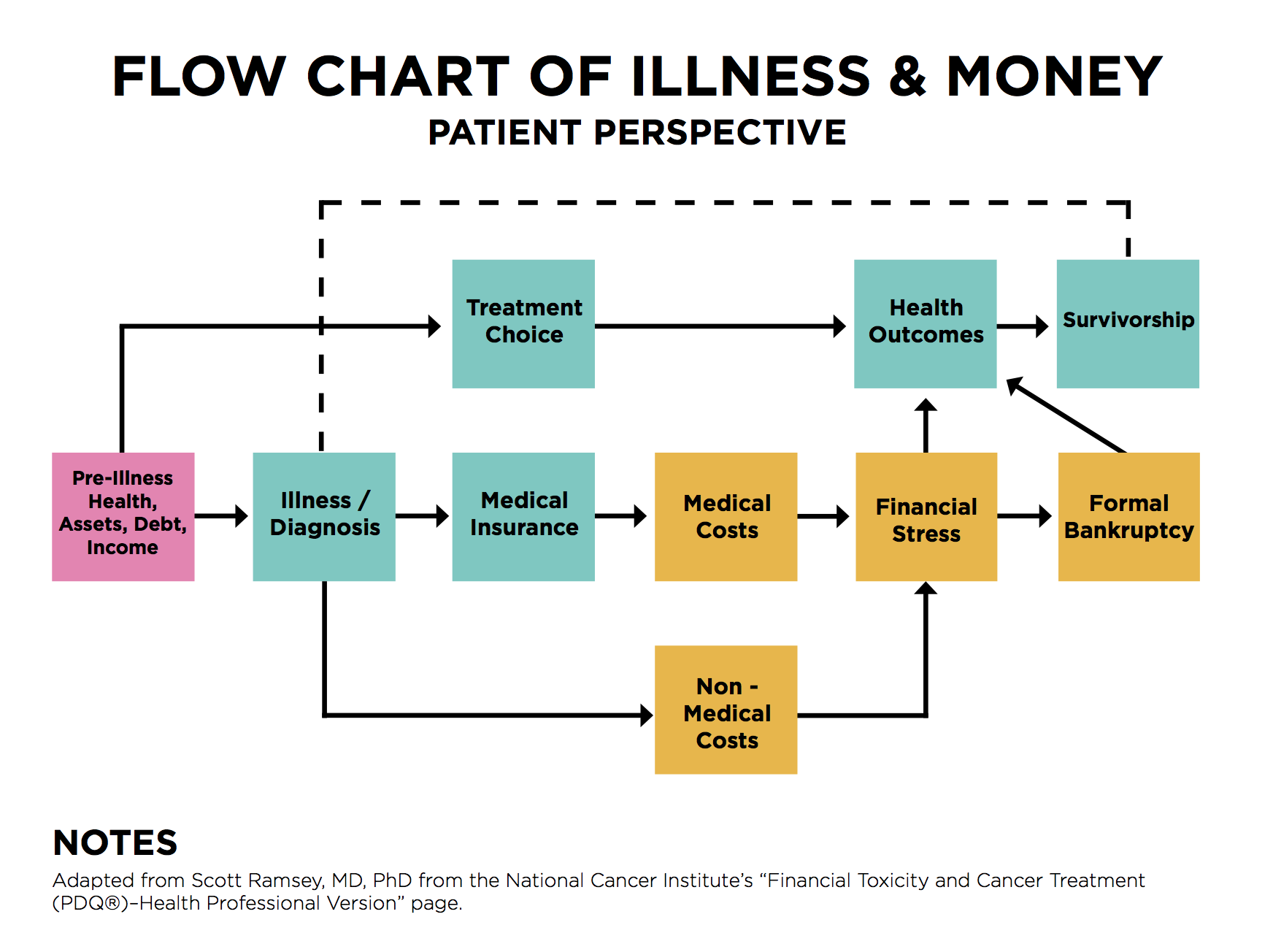
What we came up with were journey maps, key insights, and some concepts. We were encouraged not to prototype, as MSK was looking more at the research than anything else. As a result, our findings and presentations were focused more on mapping the scene than the ideas shown below.




Through it all, we met some amazing people doing some amazing things in cancer care. From those working with immigrants and those typically overlooked, to survivor’s battling to change the hospital from within, there are some amazing, beautiful people who work at and with MSK.
While we did some interesting work that I hope will give the Design team some leverage to continue working in the space, what I did notice was that I felt like I was designing in a vacuum. While we did get to talk to some patients, I didn’t feel like we talked to enough. And the fact that the cost of care is so linked with insurance made for a feeling that there was an elephant in the room we couldn’t discuss. While I understand designing within what you can change, I think limiting us to just taking health insurance as it is was a misstep. What would it look like if the hospital didn’t take insurance? How might MSK band with other NYC hospitals and demand a certain level of care for all?
These questions put a lot of responsibility on a hospital itself, so I understand a company’s urge to not do so. But in a world where adversity, inequity, and health problems are growing by the day, if our doctors aren’t able to, then who is?
Essentially, TD got me looking at large systematic changes at the root rather than designing solutions to its problem. TD! What have you done to me now?!